Have you ever wondered what the right stool shape should be?
Although it may seem like an awkward question that you may be ashamed to ask your Physician, it is still a legitimate question.
And medically important, too.
That's right, because human stool can indicate a lot about a person's health status, and their observation can detect a lot of useful information as well as be alarm bells of certain pathological conditions, both of the colon and the anorectal canal.
So, if you're wondering what shape healthy stools should be, you're on the right page.
Continue reading this informative article written by Dr. Luisella Troyer, Proctologist Surgeon, to find out what well-formed stools should be and what the 'red flags' might be that should prompt you to perform a proctological examination.

The color of stool is the result of bacterial fermentation of bilirubin, a waste product of metabolism that is part of bile.
Bilirubin, itself a decay of biliverdin, is not soluble in water and therefore the liver, to excrete it, directs it into the intestines.
There, bilirubin is attacked by bacteria in the microbiota, which transform it into stercobilin, which is what gives stool its classic brown color.
Any alteration in this natural process changes the color of the stool, which therefore can highlight both liver and intestinal problems.
Before we begin, a brief review of the human gastrodigestive system
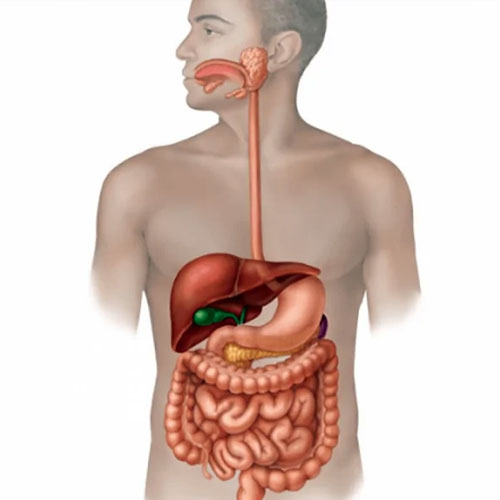
The human gastrodigestive system is that long tube composed of numerous organs that enables our body to assimilate energy and nutrients necessary for our survival, through the mechanism of digestion.
Like all other animals, Homo Sapiens is a heterotrophic living organism, that is, unable to synthesize the energy and chemical elements essential to its metabolism from nonorganic compounds, such as sunlight or minerals.
To sustain himself, therefore, man must assimilate the energy that other living beings have already produced, through regular nourishment.
The gastrodigestive system is thus the complex system of interconnected organs that serves to transform food into energy for our cells, in a long process that begins as early as chewing.
The food, crushed by the teeth and kneaded by saliva, becomes the bolus, which is swallowed and sent toward the esophagus and then the stomach.
In the stomach, the bolus is mixed and shredded, as well as chemically attacked by gastric juices: acids that kill any bacteria that may be present in the bolus and begin to break it down chemically, turning it into chyme.
Through the duodenal valve, chyme enters the duodenum and thus the small intestine-a very long tube with a peculiar internal mucosa composed of countless intestinal villi.
The intestinal villi absorb nutrients from the chyme, which are then sent to the bloodstream and the liver, which will use them to 'build' the molecules that the body's cells need for their metabolism.
After its long journey through the small intestine, the chyme, now depleted of all nutrients but still laden with fluids and electrolytes, is released into the large intestine, also commonly called the colon, through the ileocecal valve.
From there, the chyme, which has now become chyle, travels throughout the colon propelled by the mechanism of peristalsis (a synchronized contracture of the intestinal mucosa), where the lymph vessels present absorb all the remaining fluids and electrolytes, feeding them into the venous circulation.
Gradually as the pound advances in the colon, it not only 'solidifies' but is also attacked by a large amount of bacteria that live symbiotically with our intestinal mucosa, called the colon microbiome.
These bacteria, our friends, attack the residual polysaccharides (the undigested sugars) in the chyle, as well as other liver waste substances, and ferment them through their metabolism.
This fermentation permanently transforms the kilo into the alvo, that is, stool ready to be excreted.
Precisely because of the action of the gut microbiome, our stools, when healthy, are soft and easy to excrete, brown in color (of various shades) and not excessively smelly.
What are feces?
Feces, or stool, is the biological residue of our metabolism, that is, the waste nutrients that our body gets rid of through the mechanism of defecation.
They are mainly composed of fiber, that is, elements that cannot be assimilated by our intestinal villi, a very small part of water, and, for a large part, by bacterial fermentation of the intestinal microbiome.
bacterial presence in stool is really high: about 70% of the total mass of the waste is in fact composed either of bacteria or the material of their fermentation.
As mentioned a little above, stool is formed in the colon by reabsorption of chyle fluids and bacterial fermentation that is the result of the intestinal microbiome.
When they are still present in the colon, just before they are expelled, the feces have the scientific name of alvo.
The alvo, pushed toward the anal outlet by the movement of intestinal peristalsis, gathers roughly at the junction of the rectum with the sigma, where there is a natural ectasia (bulge) of the mucosa called the rectal ampulla.
This ampulla, as the name implies, fills with the formed alvus ready to be expelled, and it is precisely this dilation of it that gives us the urge to defecate.
The amount of feces produced by human beings is extremely variable, and largely follows dietary habits and, secondarily, also those of ethnicity.
On average, an adult in European or North American salutations produces about 150gr of feces per day, but this average should, for the sake of argument, be taken only as a generic guideline, variations to this statistic being very common.
What should healthy stool look like?

To the eye, healthy stools, in a nonpathological subject with good bowel activity, appear cylindrical in shape, with a smooth or otherwise only slightly 'rippled' surface, fairly long, soft, and brown in color.
On the 'degree of brownness' some flexibility of judgment must be considered: it varies greatly depending on the activity of the gut microbiome and also depending on what is eaten.
Thus, the let's say 'healthy' color of feces is a shade of different degrees of brown: a little darker or a little lighter, varying as the diet changes.
An intestinal problem, and often one external to the intestines, can only be suspected when the stool turns yellowish, too pale, completely green, or too dark, almost black in color.
In such cases, a digestive or liver problem should always be suspected, and specialized investigations should always be carried out.
Fecal smell should also be evaluated: healthy feces from a healthy adult subject should not be excessively smelly or too 'pungent'.
When this happens, there is suspicion of acidification of the alvus or an intestinal disorder (e.g., bacterial enterocolitis).
What shape should normal stool be?

In order to assess stool shape by scientific method, a general rating scale, called the Bristol scale, has been produced over the years.
This scale spans seven types of feces:
- Constipated stools, the stools are very hard, clustered in balls with the consistency termed 'goat', which are extremely difficult to expel;
- Dehydrated stools, stools are roughly formed, no longer ball-like, but still very hard to excrete, with numerous ripples on their surface;
- Formed, but slightly dehydrated, salami-like feces, however convenient to expel;
- Normoconformed, smooth, cylinder-shaped stools that are soft and easy to excrete;
- Very soft stool, not fully formed, expelled often in pieces;
- Very soft, almost liquid, mash-like feces;
- Completely liquid stools, typical of dysentery
Normal stool, that is considered physiological, are those of type 3-4.
Types 1-2 are stools typical of the condition of constipation, while stools 5, 6 and 7 are progressively more and more liquid, a typical condition of diarrhoea.
Chronic constipation, i.e., difficulty in expellingsoft, well-formed stools on a regular basis, is a serious and disabling condition that can go so far as to systematically worsen quality of life.
Constipation forces days without natural defecation, resulting in hyper-absorption of fluids in the bowel, which becomes extremely hard and difficult to expel.
In turn, such hard stools damage the delicate anorectal mucosa, sometimes even tearing and inflaming it, thus giving episodes of proctitis or actual anal fissures.
By straining to expel the hardened stool, the patient also increases intra-abdominal pressure, and this is the most common cause of the onset of hemorrhoidal disease.
Is it normal to strain to expel very hard stool?
No, it is not normal.
Punting, that is, the act of 'pushing' to allow the sphincter muscles to relax and open the anus, should not be strenuous or painful.
The feces should come out easily, and should not cause discomfort, pain or bleeding.
If you experience difficulty in expelling stools that are too hard, almost 'rocky', it means that the stool has remained in the intestines beyond the time necessary for its formation, and thus has been excessively emptied of fluids.
It is a typical condition of constipated people, that is, those suffering from the disease of chronic constipation.
Constipation, besides being disabling and giving great pain during defecation, damages the anorectal canal and is one of the triggers for anal fissures, pathological hemorrhoids, and anorectal mucosal prolapse.
Why do I always have very soft and poorly formed stool?
Poorly formed, excessively 'soft' stool that are excreted in noncylindrical pieces, sometimes almost liquid, identify an intestinal problem of liquid malabsorption of the chyle.
This malabsorption can be due to a long list of diseases and pathological conditions of the colon, for example:
- Irritable bowel syndrome;
- Celiac disease;
- Lactose intolerance;
- A bacterial or viral infection of the mucosa of the colon;
- A chronic agitative state with great stress;
- Incorrect diet;
- Ulcerative rectocolitis;
- Crohn's disease
As can be seen from the list, the alvus dysfunction that tends not to make stool form properly has a long list of causes, which must be carefully evaluated at the history during the colonproctological examination.
Should one take a bowel movement every day?
Ideally, the evacuation of a healthy, adult subject should occur on a daily basis, with the expulsion of soft, well-formed stools that are the right color brown and not excessively foul-smelling.
However, this condition often does not occur in all humans, and alterations to normal daily defecation may be common and present without resulting in a pathological condition.
Some perfectly healthy individuals, for example, evacuate twice a day, while others evacuate every other day without experiencing the typical symptoms of chronic constipation.
Only when evacuations are difficult once in four times, and roughly one is able to evacuate less than twice a week, can one begin to hypothesize a constipated condition, which must be addressed with the proper bowel rehabilitation course.
What is the danger of not evacuating for many days?
The longer the alvo remains in the intestine, the more the lymph vessels in the intestinal mucosa absorb all its fluids, thus causing it to become dehydrated and, of course, over-hardened.
The more the alvus hardens, the more difficult it becomes to expel during defecation, which often causes severe pain and tearing of the delicate anorectal mucosa.
Pathological hemorrhoids, i.e., prolapse of the hemorrhoid plexuses, is also often due to the intra-abdominal hyper-pressure that the constipated patient is forced to perform in an attempt to expel stool that has become too hard.
If evacuation is not carried out for a long time, indicatively for 5-6 days, there is a risk that the alvus, which has now become the consistency of a real stone, will obstruct the rectal ampulla, forming a kind of 'plug', which does not allow the new alvus formed in the initial tracts of the intestines to exit.
This plug is called a fecaloma, and it is a dangerous condition that can lead, without prompt intervention, to the formation of a true intestinal blockage.
Fecaloma is treated urgently with the administration of large amounts of warm water enemas and, in some cases, the necessary manual maneuver of mechanical removal of the fecal plug.
That is why one should never get to the condition of possible fecaloma, and proper bowel rehabilitation should be started to treat the condition of chronic constipation.
Are periodic enemas for evacuation harmful?

The use of laxatives and enemas should always be avoided, or used only as a last resort, just to avoid the risk of fecaloma.
Purgatives and laxatives acidify stools, irritate the intestinal mucosa and inflame it, and also damage the colon microbiome.
The habit that many ethical patients have, which is more of a necessity than a habit, of evacuating only with the use of enemas or purgatives, is deleterious and harmful.
Chronic constipation must be treated by appropriate bowel rehabilitation, which almost always requires a change in eating habits as well as medical and physiotherapeutic procedures to allow the colon to resume its proper activity.
Stool too hard and difficult to expel? Get help from Dr. luisella troyer

Dr. Luisella Troyer is a Proctology Surgeon who can help you with chronic constipation and particularly hard stools that are difficult to evacuate.
At her clinic in Dubai, Dr. Troyer can help you understand the source of your defecation problems, and can begin to treat your intestinal sluggishness with effective rehabilitation protocols.
your proctologist surgeon of excellence in Dubai

Dr. Luisella Troyer is an italian Vascular Surgeon, specialised in Proctology and Colonproctology, operating in Dubai.
In the modern, well-equipped clinic in Dubai, Dr. Troyer provides specialist medical examinations in Vascular Surgery and Colonproctology, to diagnose and solve proctological problems such as:
- Pathological haemorrhoids;
- Haemorrhoidal thrombus;
- Anal fissures;
- Anal warts;
- Peri-anal abscesses and anal fistulas;
- Chronic constipation;
- Irritable Bowel Syndrome;
- Faecal incontinence;
- Rectocele;
- Descending perineum syndrome
In the clinic in Dubai, Dr. Troyer also performs minimally invasive treatments, such as the treatment of prolapsed haemorrhoids with the innovative sterilised air-stabilised scleromousse.
For her proctological diagnoses and examinations, Dr. Troyer uses the excellence of diagnostic technology, such as the modern high-definition videoproctoscope for Electronic Endoscopic Videoproctoscopy.
All operators and assistants of Dr. Troyer speak English, Arabic and Italian.

So remember...
- DIGESTION IS THE PROCESS BY WHICH WE HUMANS ASSIMILATE ENERGY AND CHEMICAL ELEMENTS ESSENTIAL TO OUR SUBSISTENCE;
- HUMAN BEINGS ARE HETEROTROPHIC ORGANISMS, SO THEY ARE FORCED TO TAKE ENERGYAND NOURISHMENT FROM OTHER LIVING ORGANISMS;
- THE HUMAN BEING'S NOURISHMENT IS INDISPENSABLE FOR HIS SURVIVAL;
- DIGESTION IS CARRIED OUT THROUGH THE COMPLEX GASTRODIGESTIVE SYSTEM, WHICH BEGINS AT THE ORAL CAVITY AND ENDS AT THEANAL ORIFICE;
- THE WASTE PRODUCTS OF OUR METABOLISM ARE FECES, WHICH WE GET RID OF THROUGH DEFECATION;
- A HEALTHY, ADULT HUMAN BEING PROCURES AN AVERAGE OF 150GR OF FECES PER DAY, BUT THIS FIGURE CAN VARY WIDELY;
- FECES ARE FORMED IN THE COLON, AFTER RESIDUAL NUTRIENTS ARE REABSORBED OF FLUIDSAND ELECTROLYTES;
- THE BACTERIA IN OUR INTESTINES COMPLETE THE DIGESTION, FERMENTING THE RESIDUAL SUGARS FROM OUR FOOD AND TURNING IT INTO ALVO;
- THE SHAPE OF A HEALTHY HUMAN BEING'S STOOL IS CYLINDRICAL, WITH A SMOOTH SURFACE AND A BROWN COLOR;
- FECES SHOULD BE WELL FORMED BUT SOFT TO EXPEL, NOT EXCESSIVELY SMELLY;
- STOOLS OF 'GOAT' CONSISTENCY , HARD AND DIFFICULT TO EXPEL ARE TYPICAL OF CONSTIPATED INDIVIDUALS;
- STOOLS THAT ARE NOT WELL FORMED, TOO SOFT OR EVEN COMPLETELY LIQUID ARE THE HALLMARK OF DIARRHEA;
- ENEMAS AND LAXATIVES SHOULD BE USED ONLY AS AN EXTREMA RATIONEISEVERE CASES OF CONSTIPATION, TO PREVENT THE FORMATION OF A FECALOMA

This article was revised and updated by Dr. Luisella Troyer on:
Tuesday 4 February, 2025
Dr. Luisella Troyer is a Vascular Surgeon, specialising in Vascular Surgery and Proctology.
Since her training as a resident, Dr. Troyer has been interested in the study and treatment of proctological pathologies, especially haemorrhoids and haemorrhoid prolapses.
In the course of his practice as a Surgeon, he has accumulated about 5000 operating theatre hours as a first operator, of which about 120 were Milligan-Morgan haemorrhoidectomies.
He is one of the first Doctors to have studied and experimented with scleromousse therapy for pathological haemorrhoids, which he has judged to be the treatment of choice for the non-traumatic treatment of haemorrhoidal prolapses, with resolution statistics of over 95% and therefore often comparable with surgical access.