



Are you a lover of anal sex, and do you practice it periodically and regularly?
Since the dawn of Homo Sapiens evolution, anal relationships have always existed and, although sometimes stigmatized by societies of the period, they are nonetheless common to any historical context.
This article, written by Dr. Luisella Troyer, is not meant to be judgmental about your sexual preference, nor is it meant to be notional: it is only meant to help you understand the possible physiological risks of practicing anal sex so that you can choose freely and with the right health information.
For your well-being, being fully aware of your body.

It is common practice among anal sex lovers to provide evacuative enemas before intercourse, so that the partner will find a 'clean environment' before the sexual act.
In reality, this practice is absolutely deleterious, as it goes on to remove the natural protective layer of mucus, the only true defense of the anal mucosa, thus worsening the risk of inflammation and infection during intercourse.
Enemas before anal sex should therefore be avoided, remembering that it is a natural fact that small amounts of feces and mucus are present in the anorectal canal.
What is the anorectal canal?
The rectum is the last part of the digestive system, that is, the long tube that runs from the mouth to the anal orifice, allowing humans (and mammals in general) to take in the nutrients essential to their sustenance.
In fact, in contrast to, for example, plants, we mammals are heterotrophic organisms, and we're unable to synthesize all the chemical elements imperative for our metabolism, but we must compulsorily take in externally, with food, which is nothing but energy already produced by other living beings.
The gastrodigestive system is precisely that apparatus, made up of several organs, that chemically breaks down nourishment and assimilates it, allowing our bodies to survive.
There are many organs involved in the digestive system, and the large intestine, more commonly called the colon, is the least of them.
The main function of the colon is to reabsorb the fluids and electrolytes of food now deprived of nutrient compounds from the small intestine, and excrete the waste in the form of feces (stool).
To do this, the colon is completely enveloped by very thin lymph vessels, the chyliferous vessels, which, during the transit of chyle (the nutrient-poor food), absorb water and electrolytes and slowly transform it into alvo, that is, stool.
The colon is composed of five parts: the ascending colon, which begins at the ileo-cecal valve; the transverse colon, which runs horizontally through the entire abdomen; the descending colon; the sigma (with the typical sigma shape, to be exact); and the rectum, so called because it is straight.
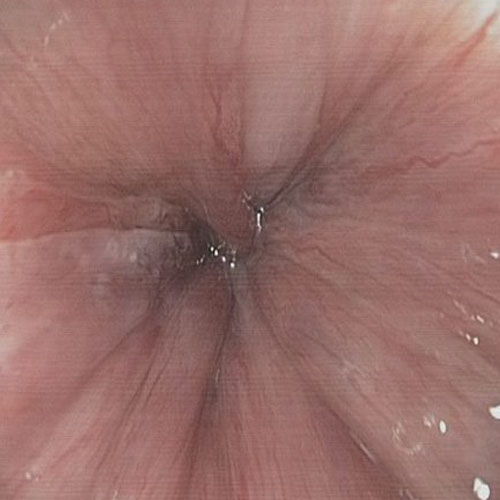
The rectal canal has an average length of about 10cm (but varies from person to person), and it flows, in the last 3cm or so, into the anal canal, which is its very last part that then opens into the anal orifice.
The junction between the rectal and anal canal is called the pectinate line or dentate line because the mucosa that makes it up has the classic vertical pleating, similar in fact to a comb.
The ano-rectal junction of the pectinate line is quite important anatomically, as it determines the point of sensitivity of the human body.
In fact, beyond the pectinate line and in the direction of the rectal canal, there are few or no pain receptors, and therefore we are insensitive to any stimulus.
From the pectinate line toward the anal orifice, however, the area is richly innervated, and is therefore hyper-sensitive to any stress.
It is precisely this hyper-sensitivity of the anal canal that is one of the reasons why, for millennia, it has also been used sexually, in the practice of anal sex.
What is meant by anal sex?
Anal sex is defined as any sexual practice that involves, to any extent, the anal orifice and/or the anorectal canal.
Due to the aforementioned massive presence of nerve endings and its proximity to other organs (both the vagina in women and, in men, the prostate), the anal orifice and anal canal are considered erogenous zones, and for this reason used, since ancient times, for a wide variety of sexual practices.
Usually, the anal orifice and anus can be used for a wide variety of oral sex practices or used for penetration, either with a penis or with manual stimulation or with the help of artificial penises (so-called dildos).
Contrary to popular belief, anal sex is not the prerogative of homosexual people: a considerable amount of heterosexual people regularly practice this sexual act, whether they are male or female.
What risks are there in practicing anal sex?

The anorectal canal is composed, internally, of tissue called mucosa, which is basically the same as that of the remaining intestine.
The anorectal mucosa, not unlike the oral mucosa, is a tissue similar to the skin, but differing from it in one important lack: the superficial epithelial layer.
Unlike the outer skin of the body, which has three layers (epidermis, dermis and hypodermis), but mucosa totally lacks the superficial one, called epithelium and part of the epidermis.
The epithelium, also called the stratum corneum, is a hard, nonvascularized layer made up of several sublayers of keratin scales: an elastic and very ductile protein produced by keratinocytes that also makes up our hair and nails.
The strange horny layer protects the delicate dermis from external attacks, both chemical and microbial, and forms, together with what is called the acid mantle, a true protective layer that is almost impenetrable to viruses and bacteria.
The anal mucosa, lacking epithelium, does not have this natural protection, and is therefore much more delicate than the outer skin.
This delicacy of it is partly compensated for by the production of mucus, directly from the muciparous glands, which are present in large quantities in the anorectal canal.
Mucus production, however, is not comparable to the natural protection of skin endowed with epithelium, and thus it is easy for the anorectal canal to be delicate and rather prone to inflammation, redness, and sometimes infection.
Having specified this, it is implicit to guess that any practice that may injure or otherwise traumatize the anorectal mucosa carries an inherent risk, which can never be entirely avoided.
Anal sex is therefore a risk in itself, regardless of how it is practiced and all the care that can be put in place to avoid injury or infection, as mentioned never fully predictable or avoidable.
Injuries and micro-injuries of the anorectal canal during anal penetration: what risks do they pose?
Anal penetration is that sexual act where one partner, male or female, penetrates the other partner anally, with the penis or its surrogate (a strap-on dildo).
This is an unnatural act for the anorectal mucosa, putting great pressure on the entire anal and rectal canal, which was not designed for this purpose.
Anal penetration is different from vaginal penetration: the vagina is an anatomical part specifically designed for sexual reproduction, and therefore its mucosal walls are exceptionally elastic as well as well lubricated by vaginal fluid.
The micro-environment of the vagina is also slightly acidified so as to kill most bacteria and viruses that attempt to penetrate the vaginal mucosa.
In contrast, all these conditions, which are essential for safe intercourse, are absent in anal sex.
The anal mucosa is not protected or lubricated by vaginal fluid, but only by a thin layer of mucus that is totally insufficient to ensure adequate lubrication during penetrative intercourse.
The mechanical stress that the anorectal mucosa can withstand is infinitely less than that for which the vaginal mucosa is designed, and therefore there is a high risk of tearing during intercourse.
These tears can be microscopic or larger, and can lead to bleeding, inflammation, or even facilitate bacterial and viral infections.
Yep, because an injured mucosa, even with micro-lacerations, is a prime gateway for pathogenic microorganisms that can be exchanged with the partner during sexual intercourse.
Just think of two fairly infectious microbes that fall into the broad category of STDs (sexually transmitted diseases): syphilis, and HIV.
In addition to infections, micro-lacerations inflame the anal mucosa, making it hypertrophic and congested, with conditions often resulting in painful proctitis (inflammation of the anorectal canal).
Larger, more extensive lacerations and wounds, which are always possible during anal intercourse, especially if violent and not well lubricated, can cause suffering of the internal sphincter of the anus, which in turn can give rise to unpredictable spasms, worsening the vascularization of the anal area and turning the wound into a painful and chronic anal fissure.
The risk of anal micro- and macro-injuries during penetrative intercourse are always present, and although proper and continuous lubrication can reduce the risks, they are never completely 100% avoidable.
In addition to lubrication, the size of the member or otherwise of the dildo used for intercourse, the duration of intercourse, and, of course, the force with which the act is performed, all contribute to the risk of anal canal injuries.
Sexually transmitted diseases with anal sex
In addition to lesions of the anorectal mucosa, there is another danger during anal sex: infections caused by bacteria, parasites, and viruses.
Infections transmitted through sexual intercourse are medically called sexually transmitted diseases (STDs).
They have been known to humans for millennia, and have plagued every type of society or ethnicity for millennia, enforcing Homo Sapiens' natural propensity for sexual polygamy.
The microbes that cause STDs are all microorganisms that spread infection through direct contact between the two partners, which normally occurs, playfully, during sexual intercourse.
Some pathogens, such as HIV, are transmitted not through skin-to-skin or skin-to-mucosal contact, but through contamination of sperm and vaginal fluids.
Still others are microscopic parasites that prey on host resources, such as scabies mites or pubic lice, known as crabs.
Among the many STDs with anal sex, it is worth mentioning the most well-known and important ones:
- ⁃ Gonorrhea, caused by the bacterium Neisseria gonorrhoeae;
- AIDS, caused by the HIV virus;
- Syphilis, caused by the bacterium Treponema pallidum;
- Ano-genital warts and anal cancer, caused by the HPV virus;
- Viral hepatitis B and C, caused by HBV and HCV viruses;
- Anal candidiasis, caused by the fungus Candida Albicans;
- Scabies, caused by the mite Sarcoptes scabiei;
- Pubic pediculosis, caused by the infestation of pubic lice Pthirus pubis known as crabs
This is just a short list of all STDs: there are many more, and potentially any pathogen that is transmitted through direct contact between two people is a candidate to join the long list.
It is worth mentioning that due to the propensity for hyper-absorption of the anorectal mucosa, the lack of the stratum corneum or in antiseptic vaginal fluid, as well as the very common presence of micro-lacerations during the penetrative act, many of the STD infections are much more likely to occur in anal sex than in traditional sex.
Anal sex practiced orally is also dangerous

Anulingus, also known by the English term rimming, is the sexual practice in which one partner stimulates the other partner's anus through the tongue.
Basically, it is the anal version of connilingus, and as such it is a form of oral sex that, in turn, falls within the range of STD infection risks.
Indeed, if in penetrative anal sex the risks of infection can be not zeroed out but at least reduced by the proper use of a condom, in rimming this is impossible, and direct contact between tongue and anus is always 'naked', without any protection.
All the major bacterial, parasitic and viral diseases already mentioned just above, including HPV infection, syphilis and hepatitis, are easily transmitted by rimming.
Fist fucking and damage to the anorectal canal and sphincters
In contemporary parlance, fist fucking or fisting refers to sexual stimulation of the vagina or anorectal canal with an internal hand.
It is a sexual practice defined as extreme, with known modern connotations but presumed to have also been practiced in the past by more ancient civilizations (although there are no certain notions of it).
Medically, it is a practice that is always discouraged and considered dangerous, from any point of view and with any 'precautions' taken: the anorectal canal is not physically designed for such abnormal dilations, unlike the vagina.
Continuously practicing fisting exhausts and weakens all the supporting structures of the pelvic floor, including the sphincter muscles that regulate the opening or closing of the anal orifice.
In addition to serious risks of serious injury, usually requiring immediate surgical intervention, in fisting the continuous hyper-pressure stress on the rectal canal can lead to chronic and irreversible exhaustion of the sphincter muscles, resulting in fecal incontinence.
In addition, there are the almost certain problems of hemorrhoidal and mucosal prolapse, with conditions, in the long run, of almost complete leakage of the rectum from the anal orifice (prolapse of the rectum).
These are very unpleasant situations, always requiring major plastic reconstructive surgeries (not always fully effective), which can contribute dramatically to the patient's quality of life.
That is why such extreme practice should always be avoided.
Pegging and penetration performed by the woman

In sexual matters, pegging is defined as the practice of anal penetration performed by the woman on the man or alternately by the woman on another woman.
It is a practice, as far as is known, that is fairly recent, spread initially through a major campaign of outright marketing by a well-known sex toy manufacturer who, in the 1890s, decided to expand its business outside of same-sex couples.
Pegging is practiced with a dildo referred to as a strap-on, that is, wearable by the woman with a belt.
There are a variety of types and as many different shapes and sizes, including hollow insides, to be worn by men.
Although the dildo obviously has no pleasure nerve endings, the active partner can still have a satisfying psychological sensation in penetrating her partner.
Compared to anal sex performed with a male member, which is definitely softer than any dildo, pegging can already be very dangerous, especially if it is practiced with strap-ons of exaggerated size and/or under conditions of inadequate lubrication.
Medically speaking, any anal penetrative activity with any type of object, even specifically designed ones such as a strap-on dildo may be, is not recommended.
Anal sex is inherently dangerous, and you have to take note of that

Sexual practice using the anus and anorectal canal has been common to humans for millennia, and often has only a limited connection to sexual orientations.
There are heterosexual couples and people who, however, use the anus (either her or his) to experience pleasure and practice sexual intercourse, without necessarily escalating into homosexuality.
Having clarified this, from a medical perspective it should also be well emphasized that anal sex is an inherently dangerous sexual practice.
The human anatomical conformation of the anorectal canal is not designed, unlike the female reproductive organs, for penetrative sexual activity, especially when performed with too much force, with members or sex boys that are too large and without adequate lubrication.
But even with all possible precautions, including constant and proper lubrication, risks of trauma and injury are always possible, so there can never be, in anal sex, a totally safe condition.
From the point of view of STDs, even with the proper use of condoms and the strictest precautionary conditions, the absence of infection of any STD pathology cannot always be guaranteed.
Some viruses and bacteria, even by using thick and strong condoms, can still infect a partner, and condom use does not, just to mention, preserve against the infection of scabies mites or pubic lice (crabs).
Should one then decide to engage in rimming, this protective condition of the condom would be completely lacking, opening the way for the most dangerous direct contact, that of mucosa with mucosa.
In homosexual subjects, continuous sphincter exhaustion and prolonged pressure stimulation of the anorectal canal statistically results in a large percentage of cases of fecal incontinence or hemorrhoidal prolapse.
This is not a critical appraisal of anal sexual practice and is not meant to be an argument for controversy: it is a medical report, in good conscience, on the inherent risks of anal sex, so that those who wish to practice it are properly informed of all the risks that, from a medical point of view, may become apparent.
Are there ways to reduce the risks of tearing and infection during anal sex?

Only partially.
As mentioned several times throughout this article, anal sex has inherent risks that can never be avoided altogether.
Regardless, you can at least try to minimize complications with the following good behavioral and health rules:
- Avoid excessively long intercourse during anal penetration;
- Avoid relationships with members that are too large, or with oversized strap-on dildos;
- Use a good thickness, well-lubricated condom;
- Avoid sexual promiscuity whenever possible;
- Avoid the practice of rimming;
- Avoid applying too much force during anal penetration;
- Constantly lubricate the member or dildo during penetrative intercourse;
- Stop immediately if the partner feels any kind of pain or discomfort;
- Stop immediately if traces of blood are noticed on the member or dildo;
- Correctly and conscientiously informing your partner about your health status and sexual dating;
- Allow the sphincters and anorectal mucosa to rest for a suitable period of time between intercourse;
- Clean yourself well after every intercourse, with a mild, fragrance-free cleanser;
- If there is redness or burning of the anal area after intercourse, soothe with rice starch and a soothing cream (calendula and propolis creams are excellent);
- If you experience bleeding or if the pain and burning does not spontaneously pass after a few days, perform a specialized proctological examination
It should be remembered that moderate post intercourse-anal discomfort and itching may be physiological, and natural response of the mucosa and perianal skin to the mechanical stress that injured and inflamed it.
In non-serious cases, these symptoms recede after a few days, but where this does not occur, it is always imperative to consult a Proctologist Physician, for a specialized proctological examination.
Do you have pain, bleeding and burning in the anus after anal sex? Dr. Troyer can help you

Dr. Luisella Troyer is a Proctologist Surgeon in Dubai, who has been perfected for years in pathological conditions of the rectum and anus.
At her clinic, Dr. Troyer can help you figure out if your anorectal canal has had any major injuries after anal intercourse, which is giving you symptoms that do not go away on their own such as bleeding, pain, and itching.
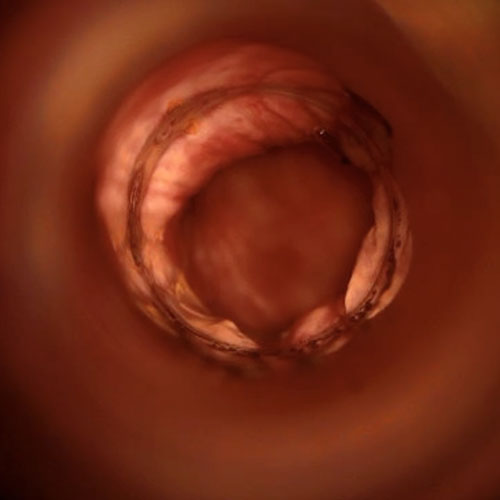
Dr. Troyer completes each proctologic examination with Electronic Endoscopic Videoproscopy: an examination of excellence that can totally assess the condition of the anorectal canal in high definition, which is essential to get an accurate and reliable picture.
Remember that the Dr. Troyer is first and foremost a Physician, sworn to protect life: this means that In her clinic you will never be judged for your sexual preferences or inclinations, but you will simply be treated.
Therefore, you do not need to have fear, shame or unfounded social fears in front of Dr. Troyer: she is here to help you be well, regardless of your personal preferences.
your proctologist surgeon of excellence in Dubai

Dr. Luisella Troyer is an italian Vascular Surgeon, specialised in Proctology and Colonproctology, operating in Dubai.
In the modern, well-equipped clinic in Dubai, Dr. Troyer provides specialist medical examinations in Vascular Surgery and Colonproctology, to diagnose and solve proctological problems such as:
- Pathological haemorrhoids;
- Haemorrhoidal thrombus;
- Anal fissures;
- Anal warts;
- Peri-anal abscesses and anal fistulas;
- Chronic constipation;
- Irritable Bowel Syndrome;
- Faecal incontinence;
- Rectocele;
- Descending perineum syndrome
In the clinic in Dubai, Dr. Troyer also performs minimally invasive treatments, such as the treatment of prolapsed haemorrhoids with the innovative sterilised air-stabilised scleromousse.
For her proctological diagnoses and examinations, Dr. Troyer uses the excellence of diagnostic technology, such as the modern high-definition videoproctoscope for Electronic Endoscopic Videoproctoscopy.
All operators and assistants of Dr. Troyer speak English, Arabic and Italian.

So remember...
- ANAL SEX IS SEXUAL INTERCOURSE PRACTICED USING A PARTNER'S ANUS;
- HUMAN HISTORY HAS SHOWN AMPLE DOCUMENTATION OF THE PRACTICE OF ANAL SEX, WIDESPREAD IN VIRTUALLY EVERY CULTURE AND CIVILIZATION;
- ANAL SEX IS NOT THE PREROGATIVE OF HOMOSEXUAL RELATIONSHIPS, BUT ALSO OF HETEROSEXUAL ONES;
- EVEN WHEN PERFORMED WITH ALL APPROPRIATE PROTECTIONS, ANAL SEX REMAINS AN INHERENTLY RISKY SEXUAL PRACTICE;
- DURING ANAL PENETRATIVE INTERCOURSE, THE ANORECTAL MUCOSA CAN BECOMEINFLAMED, INJURED, OR EVEN INFECTED WITH BACTERIA, VIRUSES, AND PARASITES;
- FOR SOME BACTERIAL AND VIRAL INFECTIONS, ANAL SEX IS THE PREFERRED ROUTE;
- THE ANORECTAL MUCOSA DOES NOT HAVE EPITHELIAL TISSUE, AND THEREFORE IS MUCH WEAKER AND MORE DELICATE THAN THE OUTER SKIN OF THE BODY;
- THE ANORECTAL CANAL IS STUDDED WITH A DENSE NETWORK OF LYMPHATIC VESSELS, WHICH MAKE THE ANAL MUCOSA VERY ABSORBENT, EVEN FOR VIRUSES AND BACTERIA;
- THE USE OF CONDOMS DURING ANAL INTERCOURSE CAN HELP DECREASE THE RISK OF INFECTION, BUT CANNOT ELIMINATE IT ALTOGETHER;
- ANAL INTERCOURSE SHOULD ALWAYS BE WELL LUBRICATED, NOT EXCESSIVELY LONG AND NOT VIOLENT
This article was revised and updated by Dr. Luisella Troyer on:
Tuesday 4 February, 2025
Dr. Luisella Troyer is a Vascular Surgeon, specialising in Vascular Surgery and Proctology.
Since her training as a resident, Dr. Troyer has been interested in the study and treatment of proctological pathologies, especially haemorrhoids and haemorrhoid prolapses.
In the course of his practice as a Surgeon, he has accumulated about 5000 operating theatre hours as a first operator, of which about 120 were Milligan-Morgan haemorrhoidectomies.
He is one of the first Doctors to have studied and experimented with scleromousse therapy for pathological haemorrhoids, which he has judged to be the treatment of choice for the non-traumatic treatment of haemorrhoidal prolapses, with resolution statistics of over 95% and therefore often comparable with surgical access.










